Listen:
-
 play_arrow
play_arrow
Can it work as 30 min? Let's see Jackie Sedley
It’s scary living in a world that expects so much of you all the time, especially for those born in female bodies.
Over 10,000 people die from an eating disorder in the United States every year. This statistic can be explored and explained through so many different lenses – looking at media, advertising, the rise of social media, society’s unrealistic expectations particularly on those born female, stigma against bodies that don’t fit the ideal, the fact that many recovery spaces don’t make room for those in bigger bodies, people of color, queer people, and those from other marginalized groups.
The bottom line: None of this will change if we don’t talk about eating disorders. When I was deep in the throes of my disorder, the guilt and shame that comes with the diagnosis made it nearly impossible to talk about it with anyone. Plus, it’s easier to give in to unhealthy behaviors if nobody knows to look out for them. But in the years since I started my recovery, at 19, I am much more willing to discuss my experiences. I think it’s important that I do.
I wanted to do this series for many reasons. I want to educate listeners about eating disorders as a diagnosis, and work to debunk some myths around what “qualifies” as an eating disorder. I’ll bring experts on to talk about fad diets, intersectionality when it comes to eating disorders, treatment methods, and more with the intention to destigmatize this topic.
I also hope people listen with an open mind. You don’t have to look a certain way, act a certain way, or think a certain way in order to address your relationship with food and body. You don’t need a diagnosis from a professional to decide you’d like to feel better in your own skin.
This episode will focus on the rates of eating disorder diagnosis in the United States, the stigmas and stereotypes that act as huge roadblocks to people getting help, and ways to navigate a world that sets us up to hyperfixate on food and our bodies.
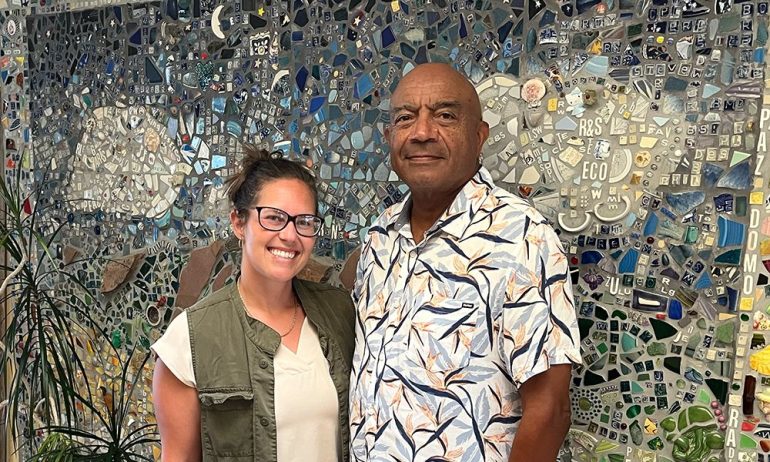
I sat down with two professionals in the world of eating disorder recovery: Stephanie Albers, a clinical assessment program manager at Project HEAL, and Terra Towne, a licensed clinical psychologist at the UC San Diego Eating Disorders Center for Treatment and Research and the program manager of their Intensive Family Treatment Program.
The episode referenced Project HEAL’s 2023 assessment of 395 individuals with eating disorders. Here’s what they found:
- The highest rates of diagnosis were for atypical anorexia, at 33%.
- The second-highest category after atypical anorexia was binge eating disorder at 17%, followed by anorexia nervosa also at 17%.
- 40% of assesses were BIPOC.
- 50% identified as part of the LGBTQ+ community.
- 18% identified as being trans, non-binary, or intersex.
- 64% of assesses were 24 years or older.
- 36% identified as having a disability or being neurodivergent.
- This stayed true when broken down by male-identifying, female-identifying, and non-binary identifying.
KGNU’s Jackie Sedley gave the timeline of their own eating disorder recovery in episode 1 of this series. You can listen to that here.
Resources:
National Association of Anorexia Nervosa and Associated Disorders (ANAD)
Families Empowered and Supporting Treatment of Eating Disorders
UC San Diego Eating Disorders Center for Treatment and Research
There are many types of eating disorders. The most commonly diagnosed are:
- Anorexia nervosa
- Binge-eating disorder
- Bulimia nervosa
- Orthorexia
- Avoidant Restrictive Food Intake Disorder (ARFID)
Transcript:
Jackie Sedley: You’re tuned in to listener-supported KGNU, this is A Public Affair, I’m Jackie Sedley, bringing you episode two of my limited series, Nourished. Every 52 minutes, someone in the United States dies from an eating disorder. That adds up to over 10,000 deaths each year. This statistic can be explored and explained through so many different lenses, looking at media, advertising, the rise of social media, society’s unrealistic expectations, particularly on those assigned female at birth, stigma against bodies that don’t fit the ideal, the fact that many recovery spaces don’t make room for those in bigger bodies, for people of color, for queer people, and those from other marginalized groups.
We can look at all of this, but the bottom line is that none of it will change if we don’t talk about eating disorders. I was diagnosed at age 17 with anorexia, and I talk about it openly now, including on our airwaves. You can hear my timeline in episode one of this series on KGNU. org.
It’s scary living in a world that expects so much of you all the time, especially for those assigned female at birth. I wanted to do this series for many reasons. I want to educate listeners about eating disorders as a diagnosis and work to debunk some myths around what qualifies as an eating disorder.
I’ll bring different experts on to talk about fad diets, intersectionality when it comes to eating disorders, treatment methods, and more, with the intention to de stigmatize and open up the conversation around the topic. I also hope people listen with an open mind. You don’t have to look a certain way, act a certain way, or think a certain way in order to address your relationship with food and body.
You don’t need a diagnosis from a professional to decide you’d like to feel better in your own skin. I gave a broad definition of eating disorders in episode one, but just to reiterate, an eating disorder is any of a range of mental disorders categorized by a preoccupation with food that negatively impacts your physical and psychological health and hinders your ability to fully engage in day-to-day life.
I think it’s really important to keep reminding listeners throughout the series that eating disorders are mental illnesses, not physical ones. They manifest in physical symptoms and behaviors, but can always be attributed to something going on mentally, or biologically, socially, or culturally. There’s always more to the story.
One thing that I didn’t touch on too much in episode one, that I will today, is the challenge of talking about eating disorders. I’ve learned that this topic can bring out some pretty intense sides of people. That’s because, I think, everyone is touched by disordered eating and negative body image in some way.
I’ve yet to meet someone that I can confidently say has never once had a negative thought, feeling, or relationship with food or their own body. If you’re listening and you really, truly believe you’re one of the few that’s been entirely unaffected, congratulations. I bet you can still learn a thing or two from the information I’m about to share.
For this second episode, I sat down with two professionals in the world of eating disorder recovery. They’re Stephanie Albers and Terra Towne. Albers is a clinical assessment program manager at Project Heal, one of the nation’s leading non profits in trying to eliminate barriers to healing relationships with food and body
whether that be through access to care or access to treatment. Tara Town is a licensed clinical psychologist at the UC San Diego Eating Disorder Center and the program manager of their Intensive Family Treatment Program.
You’ll hear from Albers first. Albers and town sound kind of similar, but I’ll keep clarifying who is who. Project HEAL, which Albers is a part of, did an assessment of 395 individuals last year and a lot of the points she brings up are based on those assessments.
You can find the data from that assessment on our website under the link to this episode.
Sedley: Eating disorders are not immune to stigmatization that you often see enshrouding mental illnesses. Media most often depict the quote unquote typical eating disorder patient as skinny, white, affluent, and female identifying. This is the swag stereotype that I’ve talked about in the previous episode.
Anorexia seems to be the most widely acknowledged eating disorder historically, both by society and by the medical industry. Project HEAL’s assessments debunk these stereotypes to a degree, simply by finding that the highest percentage of assesses were those with atypical anorexia.
Other nationwide assessments, like from the National Institute of Mental Health, point to binge eating disorder as the most commonly diagnosed. So, with those statistics in mind, can you provide any context to this prominent stereotype of anorexia? Specifically, why we categorize anorexia as a mental illness that affects skinny, white, affluent individuals who were assigned female at birth?
Stephanie Albers: That’s a good question. I think. When eating disorders were first appearing in the medical literature, those were the first folks that were being identified as having eating disorders, anorexia was in the DSM, the Diagnostic and Statistical Manual. First, I think traditionally that may have been the folks who have had access to care and therefore were able to be seen by professionals, had close surrounding community that noticed these types of behaviors in them and saw them as problematic.
Sedley: Terra, turning to you, there’s so many barriers to diagnosis based on factors like body size and socioeconomic status, race and ethnicity and sexuality even. Through your research, how have you seen these biases toward those that fit the swag mold impact individuals access to diagnosis and treatment firsthand if they do have an eating disorder?
Terra Towne: It’s a huge misconception and myth that eating disorders only affect people who fall into that category.
And just in general, that you can determine that someone has a needing disorder just by looking at them or what they might weigh. This has had a huge negative impact on access to care and identification and diagnosis. To speak on the anorexia front, only percent of people in treatment are considered medically underweight.
Now there is a diagnostic criterion for anorexia nervosa, stating that someone has to fall into that medically underweight category to meet criteria for the diagnosis. There’s a subtype of anorexia called atypical anorexia, which is used to diagnose folks who have lost a significant amount of weight, display all the cognitive and physical symptoms of anorexia, but don’t fall into that subjective category of being medically underweight. And because that the first line of detection is often in primary care, it’s often missed. Not to put any doctors down, but they just don’t have the specialized training and eating disorders. And so what we find is those folks who have atypical anorexia, their diagnosis is missed altogether.
And, at worst, their weight loss in their disorder is even praised because they may now fall in or closer to a medically quote unquote “healthy weight” or BMI. So that’s extremely problematic because atypical anorexia in no way is a subclinical disorder.
So we know that the rates of medical medical instabilities are the same as those with typical anorexia and the psychological symptoms that we see in those with atypical anorexia are actually elevated when compared to those with typical anorexia.
On the B.E.D. (binge eating disorder) front, this is really interesting. You know, when you look at it and you see that most folks who are diagnosed with BED fall into the medically overweight or obese categories, you have to think that there’s some type of weight stigma that prevented these folks from being diagnosed and treated much earlier on.
Sedley: So, so what do we do with all that? Because anorexia does have the highest recorded death rate of all mental illnesses, and by no means should that be overlooked. But if we’re thinking about the skew that certain data may have, based on under diagnoses or mis-diagnoses, how do we improve access to diagnosis and treatment for folks with all types of eating disorders? If those that get the most attention from doctors and concerned loved ones are those that fit into the SWAG stereotype and are diagnosed with typical anorexia.
Towne: This is a problem. I think that the field has tackled and simultaneously Not made, I think the changes that we need to for like decades.
So as far as like, how do we address this treatment gap? How do we get people identified and in treatment before it’s, it’s really not optimal? I think we need just better education at the level of the healthcare providers. I think eating disorder specialists really need to be consulting with physicians, since they are that first line of identification and they’re often the provider that unfortunately folks with eating disorders are having a negative experience with because they’re coming in either not wanting to share symptoms right, or sharing symptoms, but being kind of underestimated because of the size of their body or their weight.
And then I also think there just needs to be more community-wide discussions about mental health and eating disorders specifically. I think since COVID, I’ve definitely seen a shift in schools talking openly about mental health and, parents being more open to teens going to therapy, more preventative care, but I still think there’s a specific stigma around eating disorders, and somehow, and I’ve seen it in even the most educated, mental health-conscious parents is that there’s something about an eating disorder that really trips them up and feels difficult to talk about and feels like it’s a different mental illness than say, depression or anxiety.
And I think that has to do with just these misconceptions that exist about eating disorders, right? Not just who it affects, like we’ve been discussing, but also why it comes about.
Something that’s really important in the field is increasing early access to treatment for all and not getting stuck in this model of care where people need to get sick to get treatment. I think just getting the word out about the range of different eating disorder symptoms that exist and how these are treatable illnesses and issues, just like other mental health problems that teens and everyone can encounter, is going to be really, really important to making sure that everyone has the opportunity to be diagnosed and to get help.
Sedley: Hi there, Jackie Sedley here. If you’re just now tuning into KGNU, we’ve been listening to the first half of a conversation between myself, Stephanie Albers and Terra Towne. Albers is a clinical assessment program manager at Project Heal, and Towne is a licensed clinical psychologist at the UC San Diego Eating Disorder Center.
This is episode two of my limited series, Nourished, unpacking our biases against bodies and behaviors around food. We’ll jump back into that conversation now.
Sedley: Stephanie, what kind of barriers have you been made aware of through your work, or through personal experience, to just being told by a medical professional that you have an eating disorder?
Albers: I think there’s a lot of different barriers. One, you almost have to know yourself that something is wrong to be able to articulate to someone that you’d like to be screened for this, unless you’re appearing as underweight you may not ever get asked about what you eat or your activity level, unless it’s in
the context of being told you should probably lose weight. Healthcare professionals also have a stereotype of what they think a person with an eating disorder looks like.
And so you may be at your primary care doctor and it may never come to their attention to additionally refer you to be screened or should get diagnosed for an eating disorder.
And, I think if we don’t see ourselves represented in advertisements for eating disorder treatment centers, or, eating disorder care, eating disorder awareness, it’s less likely that we’re going to think that that could possibly be us. And so that eliminates that piece and potentially a health care provider may not notice it either.
Sedley: Terra, so you said people don’t need to get sick to get treatment. That’s something that you focus on a lot in your research. Can you say more about that? What does that mean to get sick? And why is it important to provide support before that level is reached? Or even if it never is reached.
Towne: Yeah, absolutely. So I think a symptom of eating disorders – and when I say eating disorders, I guess I’m talking specifically about anorexia and bulimia in this case – is that folks feel like they don’t really have an eating disorder. They may not feel like they’re deserving of getting help when in reality, they might be struggling very much with their eating disorder. So not only do we need to look at models of prevention when folks start to have feelings of dissatisfaction with their body or start to feel like they maybe need to start watching what they’re eating. But also, just letting people know that an eating disorder isn’t determined by a weight on the scale or the way that someone looks. An eating disorder is really about a mental struggle. And so if you’re someone who has anxiety around food, or is even thinking about it more than you used to, or feel like you’re spending a lot of time focusing on your weight and shape, or how your clothes fit, or how often you’re going to the gym, you deserve to talk to somebody about it.
You deserve the help that is out there and hopefully, that’s a better outcome than waiting until those symptoms are escalating , and you’re in a place where it’s even harder to make a full recovery.
Sedley: Stephanie, turning to you, how do you see an increase in online activity, especially among the younger generation, affecting rates of eating disorders or disordered eating behaviors?
Albers: I think there is a lot of normalization of diet culture and dieting within social media that a young person immediately can access.
And so someone who is going to a social media account without the intention to avoid those sort of things is going to be bombarded with them. And so I think sometimes if you haven’t had a lot of social media literacy, I think you don’t necessarily understand that, that stuff is not realistic, that that’s not feasible.
And there is also just the prevalence of like altered images and AI and beauty ideals that are not only unattainable for most of us, but the person portraying it may not even have attained that.
And so, there’s a lot of just, I think, pressure, intentional pressure, and then some stuff that’s not quite as intentional to look and appear and behave a certain way that impacts all of us, really.
Sedley: I know, Terra, that you’re also the program manager of UC San Diego’s Intensive Family Treatment Program. And so I wanted to ask, do you see a lot of patients with eating disorders that come from homes or friend groups that participate in these kinds of disordered eating or negative self talk patterns? And if so, what kind of effect can that have on the manifestation and development of an eating disorder in somebody?
Towne: So, you know, we live in a world that is massively impacted by what we call diet culture, or this phenomenon of your body, being a state of work, and it actually being like an admirable endeavor to try to work on yourself, with the goal of getting smaller.
It’s not just patients that are affected by it but it’s all of us who live in that environment. So certainly we have patients who are coming in and, their family, maybe holds some of the same beliefs that they’re eating disorder does or their friends that are dining alongside them.
It’s their coaches, their grandparents who are sending the same messaging and maybe even giving praise for some of the disorder behaviors that are being observed and that’s a big challenge for the patient because it’s a normalization of symptoms. But I do just want to make it very clear that there’s nothing in the research that indicates that parents are the cause of eating disorders.
We know that there’s a strong biological basis to these disorders. And so usually when they manifest, it’s like this combination of having this unique biology and also being in an environment where that kind of comes on.
But they can be an support person by learning more about diet culture, being more mindful of their own language, and different triggers that can ultimately serve to maintain their child’s eating disorder.
Sedley: I really appreciate that perspective. It wasn’t until I was diagnosed with my own eating disorder that I found out that there is a genetic component that family members of mine have been diagnosed with eating disorders. And so I’m very aware that that component there is very strong. I also know that the more I’ve gone through my recovery, the more I look around me and realize that a lot of people speak in ways that they don’t realize can be harmful. Maybe even from my perspective, I would go so far to say their quality of life would be improved and the quality of lives of others around them would be improved if they didn’t talk that way, or looked inside themselves and did the work and didn’t think that way. But you also can’t force somebody to change the way that they live their life, right? So, that gets tricky.
Terra, do you have any guidance or advice for folks that are living within those circles of people that maybe talk negatively about their food or body, but they also know they don’t really have a right to tell that person that they have a full blown eating disorder and that they should enter treatment because that just may not be the case or they may not be ready to hear that, somewhere in that gray area.
Towne: It’s a really tough thing, especially for those folks who are in early recovery, and they may have been in like a treatment bubble where everyone’s on the same page and is really supportive and mindful of their language around food and body, and then they’re returning to a college campus or a home where there’s a lot of talk about what someone’s eating and what people look like and things like that. So, I would always encourage patients or people in recovery to be their own advocate in those situations, whether that looks like being very confident in responding to comments like that with, “well, I don’t think of food or my body that way, or even “when I hear you say that, it makes me feel anxious about myself or like I should be doing something differently.” I also think it can be really helpful when support people are also involved in just learning about how diet culture has a negative impact on everybody. When you bring community into it, I think it can be this really beautiful dismantling of even a microcosm of the full, sort of spectrum of diet culture. It’s a really beautiful thing.
Sedley: So, Stephanie, if an individual is noticing their disordered eating patterns, but they don’t necessarily have a diagnosis in place, they’re aware there’s something going on, that they’re struggling to change, and they know their quality of life is affected as a result, what kind of guidance through Project Heal or in your personal lived experience do you provide to folks who maybe aren’t ready to take the step to move toward treatment or just simply can’t afford it?
Albers: With Project HEAL and our clinical assessment program, we do assess individuals 12 and older.
We really kind of walk folks through a series of questions about their eating behaviors, their psychosocial history and any other relevant history that might relate to their overall well being in their relationship with food.
We’re beginning to launch our Body Reborn Community Care Program. It’ll provide virtual intersectional community for those who struggle with disordered eating and have faced systemic barriers due to race those that originate for people of color. So it lasts about eight weeks and we engage in education and live discussion around systemic oppression, trauma, and their effects on our relationship with food and our body.
That can be a great place to start and you We’ll find yourself in a group and you will hear folks mention things that you’re like, oh, I thought I was the only one that thought about it this way. I think sometimes, if you’re in the throes of an eating disorder , it can be hard to navigate all the options yourself. And so, talking to others that you trust can be a good way to start as well. Simply ask them, “you know, I think I’m just not sure about this. Have you noticed anything different about me?” You know, “this is what I’m experiencing. Can you help me find help?”
Sedley: Based on my personal experience in recovery and and maybe people that are in recovery are the main ones that can relate to this. Once you start to unpack your lived experience, all of the diet culture, and the myths, and the negative self talk around the world. You can’t really stop hearing it and seeing it.
Albers: Yes.
Sedley: And, and so you start to see it in the people around you.
And the veil lifts and you realize that you really can’t think of many people in your life that haven’t been at least minutely impacted, even if it hasn’t translated to behaviors.
And so I think of the folks in my life who I wouldn’t necessarily say from my perspective have full blown eating disorders, but they have disordered eating. They can still go hand in hand, right? Very quickly. It’s a slippery slope. For those individuals that have disordered eating patterns, if you try to talk to them, often there’s resistance. So instead of trying to unpack all of that for listeners, the question I pose to you, Stephanie, as someone who is in recovery, is what are some of the most beautiful parts of your recovery for you? What do you feel like you have in your life that you simply wouldn’t have if that preoccupation with food was still there?
Albers: I can remember when I was in the throes of my eating disorder and, I had goals and interests, but they all seemed so far out of reach because I just couldn’t get out from underneath myself.
Things I wanted to accomplish, things I wanted to do were just so incredibly hard because I was undernourished. I just wasn’t physically at an optimum. And I think sometimes we think, oh, if I, lose weight or eat healthy or have a certain food or exercise regimen, all of a sudden I’ll have all this more energy.
And honestly, nothing has given me more energy than continuing to be well fed and eating regularly and nourishing myself regularly. And it’s just amazing I can read a book without losing concentration and I can, and do that.
I can carry on conversations with folks that matter to me without drifting off or getting tired. So many things that when I was in the throes of my eating disorder, I just did not have the energy for and just could not enjoy because so much of my brain space and my, My physical well being was wrapped up in the eating disorder.
I just couldn’t see, couldn’t see a way out of it. And just to realize other goals and interests that I have that don’t involve food or weight or even fitness. Like, I, I don’t spend days and hours thinking about holiday meals before I have them. And there’s just so much peace and so much room in my life for whatever wants to come into it. I think that’s probably the biggest, biggest piece of it. There was just no room for anything else in my life before.
And it’s just amazing. What has come my way since then. When you’re malnourished, you’re underfed or not regularly fed, your brain. It’s not operating on, on full power. And so I think that can really impact what it is that you see. It’s not like a hallucination, but it’s just your reality testing is not quite there. Like, it’s just not fully, fully sunk in.
I think for most people, it’s, it’s hard to realize that how you look is probably the least interesting thing about you. Like, there’s, there’s so much more to you and your person and, and how you are.
Sedley: And with just a couple of minutes left here, I wanted to ask you, Terra, if you had any resources that you wanted to highlight for listeners that are struggling, or that have loved ones that are struggling.
Towne: So for folks who are supporting those with eating disorders, whether it be parents, partners, siblings, I would definitely recommend that they check out Families Empowered and Supporting Treatment of Eating Disorders. It’s really just a wealth of information that can be helpful to anyone who’s supporting a loved one with an eating disorder. I mean, I just kind of want to end on a message of hope. There’s a lot of work to be done in the field of eating disorders, both in terms of identification for all, access to care, and improving treatments, but there’s a lot of hope here.
No matter how long somebody has been struggling, there’s really always hope for recovery. There’s been studies done that show that most people do recover from eating disorders after a period of time.
So for anybody struggling, I would just like to send a message of hope and that persistence and hope over the long term is, I think, really a huge key in getting better.
Sedley: That was me, Jackie Sedley, speaking with Stephanie Albers of Project HEAL and Terra Towne of the UC San Diego Eating Disorder Center. I tried to find statistics relating to relapse and recovery for people with all different kinds of eating disorders, but the research varied. The point I really want to hone in on though, once again, is that we cannot hope for more recovery and less relapse if we don’t keep talking about eating disorders and breaking down those stigmas.
Eating disorders are not about personal vanity. They’re not a lifestyle choice. They impact individuals of all backgrounds and identities. And throughout this series, I’ll continue to uplift the voices of those from different backgrounds and identities, from those different communities, in the hopes that we can continue to expand this conversation and reach more people who can relate to this topic.
And those that can’t, you can listen too. I’m sure you can learn a thing or two. That’s it for episode two of my limited series, Nourished. More episodes will come out later this month, so stay tuned in to KGNU.
I’m Jackie Sedley. Take care.